![]()











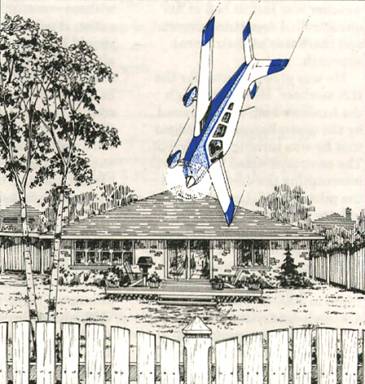
Controlled Flight Into Terrain (CFIT) at Night

On January 15, 1998, a Piper PA-31-350 Chieftain was on a passenger flight from Edmonton to High Level, Rainbow Lake, Edmonton and Calgary, Alberta. Following an uneventful flight to Rainbow Lake, the aircraft departed in darkness at 19:35 Mountain standard time on an instrument flight rules (IFR) flight to Edmonton. Shortly after takeoff from Runway 27 the aircraft collided with trees and terrain approximately 3000 ft. west of the departure end of the runway. The 9 occupants sustained minor injuries, and the aircraft was substantially damaged. This synopsis is based on the Transportation Safety Board of Canada (TSB) Final Report A98W0009.
The sky was clear with unrestricted visibility and light winds. The ambient lighting conditions were described as dark, with no moon, little illumination from the night sky and no lights to the west of the airport. The operator chartered the Piper PA-31-350 Chieftain and a pilot from another company. The company had flown the route for the operator in the past; however, the pilot had not previously flown for that operator. He had been employed as a charter pilot for approximately 6 months, held a valid airline transport pilot licence (ATPL) and had accumulated 3700 hrs of flight time, including 93 hrs on Piper PA-31 aircraft and 590 hrs at night. His background included flight instruction and charter. The majority of his charter experience was as a single pilot. He had never received formal two-crew flight training, recurrent ground training or simulator training that emphasized CFIT prevention strategies.
The operator routinely assigned two pilots to comply with the requests of a number of regular passengers and to inspire confidence. In accordance with that policy, a "co-pilot" was part of the flight, but was in fact a customer service representative, and not a flight-crew member. He assisted with baggage loading, passenger briefings and so on. He held a commercial pilot licence with an instrument rating, but did not hold a pilot proficiency check (PPC) for a Piper PA-31. The captain preferred to operate the aircraft as a single pilot, and the "co-pilot" was not assigned any formal cockpit duties.
There were no reported mechanical abnormalities with the aircraft. It was fitted with an approved supplementary device that increased the maximum permissible takeoff weight from 7000 lb. to 7368 lb. Runway 27 at the Rainbow Lake Airport is 4500 ft. long, with low-intensity runway edge lights, green threshold and red end lights and no approach lighting. It slopes uphill, and departures are accomplished into rising terrain.
Each passenger was permitted to transport a maximum combined weight of 50 lb. When the total load exceeded the gross weight of the Chieftain on any leg of the flight, it was the operator’s policy to remove the second pilot from the flight before reducing the number of passengers. Neither the chartered company nor the pilot had been advised of this policy.
The pilot completed a computer-generated flight plan and gross weight calculation, but there was no evidence that centre-of-gravity (C of G) calculations were performed. The visual flight rules (VFR) flight plan indicated that there would be a fuel stop in Peace River on the return leg. However, when the aircraft arrived in High Level, the pilot was informed that the operator did not normally stop in Peace River for fuel and preferred that the aircraft not do so in order to ensure that the flight remained on schedule. The pilot consulted with the "co-pilot" and was advised that one male passenger had been replaced with a female passenger, that most of the passengers would be travelling light, and that several of them weighed less than the standard passenger weight. The pilot amended the flight plan and added fuel to complete a VFR flight to Rainbow Lake and an IFR flight to Edmonton. A copy of the original company flight plan indicated that the pilot had originally planned to leave Rainbow Lake with 504 lb. of fuel.
Calculations completed after the accident indicated that approximately 850 lb. of fuel were on the aircraft at the time of departure from Rainbow Lake. Weight and balance calculations using estimated baggage and standard passenger weights indicated that the aircraft was at approximately 7473 lb. on takeoff from Rainbow Lake, and that the C of G was near the aft limit. Calculations using passenger self-reported weights indicated that 7 of the 9 passengers exceeded the standard passenger weight, that the aircraft was approximately 7683 lb., or about 315 lb. above the approved gross weight at takeoff, and that the C of G was about 0.35 in. aft of the aft limit.
The aircraft struck several trees with wings level in an approximate three-degree descent. It came to rest upright, and the cockpit and cabin sections remained intact; the occupant survival space was not compromised. The wings-level impact attitude, the shallow impact angle, the small tree size and the presence of approximately two feet of snow on the ground had contributed to maintaining the deceleration forces within the limits of human tolerance. The aircraft was reportedly equipped with a survival kit, as required by regulation, but investigators did not locate the kit in or near the aircraft.
Aircraft using Rainbow Lake airport typically take off from Runway 09 during night departures if the wind conditions permit, as several lights are visible to the east then. On arrival at Rainbow Lake, the pilot had been advised by the "co-pilot" of a minor frost heave in Runway 09 near the runway threshold. To avoid the risk of damaging the nosewheel during takeoff, the pilot elected to depart on Runway 27.
The pilot selected 10° of flap for takeoff and rotated at 85 kt. indicated airspeed (IAS). He believed that the aircraft became airborne at 90 kt. approximately halfway down the runway, and that he had established and maintained a positive rate of climb. He reported that he was waiting for the aircraft to accelerate to the "blue line" speed (best single-engine rate of climb) of 107 kt. IAS prior to lifting the flaps when the aircraft struck the trees. The landing gear and the flaps were in the UP position at impact.
Soon after liftoff, the pilot was confronted with dark, featureless terrain. Darkness and the absence of external visual clues may induce a false perception of altitude and attitude. Under acceleration, the combination of gravity and inertial forces produces a resultant force at an angle aft of the true vertical. This force, acting on the vestibular system of the human inner ear, can give a false pitch-up sensation. While the aircraft may be flying straight and level or climbing slightly, pilots may have a sensation of climbing at a much steeper angle than they actually are. Without visual input to override the false sensation, the pilot will usually pitch the aircraft’s nose down to correct the perceived steep climb, and inadvertently descend. This form of spatial disorientation is known as the "false climb" or somatogravic illusion. The extent, if any, to which somatogravic illusion contributed to this accident was not determined.
The TSB’s analysis focused on the pilot’s applied IFR/night takeoff technique, the role and influence of the "co-pilot," the communications between the chartered company and the operator, the request to change the flight plan, and the effect of the overweight condition of the aircraft on the departure. Individually, these factors would likely not have been significant enough to cause an accident. When combined with dark ambient conditions and an uphill takeoff toward rising terrain, these factors collectively established a window of opportunity for an accident to occur.
The pilot’s night departure technique is considered to be the active failure in this accident. Night departures in dark conditions require full use of the aircraft flight instruments, and it is essential that the pilot achieve and maintain a positive rate of climb. In the absence of outside visual cues, the pilot must rely on the aircraft instruments to maintain airspeed and attitude and to overcome any false sensations of climb. The pilot was either relying on outside visual cues during the initial climb and/or using only a partial instrument panel scan while being influenced by the false-climb illusion. Pilots can overcome false sensations by flying the aircraft with reference to the altimeter, vertical speed indicator, attitude indicator and airspeed indicator, which, in this case, would likely have allowed the pilot to detect that the aircraft was not in a climb. The appropriate technique would have been to climb at the aircraft’s best rate or best angle-of-climb speed until above all obstacles rather than become preoccupied with reaching blue line.
The role of the "co-pilot" is somewhat ambiguous, and his presence does not appear to have contributed to the safety of the flight. Because he was not familiar to the captain and because he was not delegated flight-crew responsibilities, his participation during the flight created a situation of crew resource mismanagement. The co-pilot’s remarks regarding the weight and flight-plan changes at High Level appear to have encouraged the captain to cancel the planned fuel stop in Peace River. The co-pilot did not advise the captain that, if weight was a concern, he could remain in Rainbow Lake. The co-pilot’s apparent well-intentioned advice on the frost heave near the threshold of Runway 09 influenced the captain’s decision to take off on Runway 27, which was uphill toward rising terrain and with no lights visible after departure.
The estimated weight of the aircraft at takeoff, which was approximately 315 lb. above the prescribed increased gross weight, and the C of G, which was at or beyond the rear limit, would have increased the takeoff distance and reduced the climb performance of the aircraft. The request to the captain in High Level to add fuel in order to avoid a stop at Peace River contributed to the aircraft’s being overweight on departure from Rainbow Lake.
Communication between the operator and the chartered company with regard to the duties of the co-pilot and the weight of the aircraft at departure from Rainbow Lake were inadequate. Both companies were familiar with Piper PA-31-350 capabilities, and the weight and balance calculations performed prior to the aircraft’s leaving Edmonton indicated that the trip would have to be accomplished VFR, with a fuel stop at Peace River, to accommodate the passenger load. Critical information, such as the option of dropping the co-pilot in the event of an overweight aircraft condition, was never provided to the chartered company. The pilot, who was the final decision-maker, was put in the position of having to balance the conflicting objectives of operating the aircraft within the prescribed weight limits and satisfying the customer’s demands. He was relatively inexperienced on Piper PA-31-350 aircraft, having flown less than 100 hrs on the type, and, because he had not previously flown for the operator, he was unfamiliar with its daily flight routine.
The TSB determined that the aircraft was inadvertently flown into trees and the ground in controlled flight and dark ambient conditions during a night departure because a positive rate of climb was not maintained after takeoff. Factors contributing to the accident were the pilot’s concentrating on blue-line speed rather than maintaining a positive rate of climb, the dark ambient conditions, a departure profile into rising terrain, an overweight aircraft and crew resource mismanagement.
Fizzled by Freezing Drizzle

We often discuss the dangers of flight in freezing precipitation, but we have relatively few documented occurrences in which it played a critical role. The following event, based on the Transportation Safety Board of Canada (TSB) Final Report A97O0032, provides us with such a chilling tale.
A Cessna 208B Caravan departed on March 4, 1997, from Hamilton, Ontario, on an instrument flight rules (IFR) cargo flight to Barrie–Orillia (Lake Simcoe Regional) airport at 07:15 Eastern standard time (EST). The flight, flown at 5000 ft. above sea level (ASL), was approximately 15 NM southwest of the airport on a radar-vectored heading to the airport. The pilot, who was alone on board, descended to 3000 ft. ASL and flew a full VOR/DME approach. When he got closer to the airport, the pilot was asked on the radio by a company employee if he was going to land, as the weather conditions were marginal. He replied that he would know in just a moment, and then almost immediately reported on left base for Runway 28. The aircraft crashed moments later, fatally injuring the pilot.
The aircraft struck the ground while in a steep, left-banked, nose-down attitude. Initial impact was with the left wing tip, 240 ft. short of the threshold of Runway 28. The ground scar from the wing tip was in line with the runway centreline, with the wreckage trail on a 330°M heading.
Mixed rime and clear ice accumulations were found on the unprotected leading edge surfaces of the aircraft; however, the parts protected by anti-ice equipment were mainly free of ice. The larger pieces of the broken windshield had ice adhering to them, while the heated portion of the windshield anti-ice panel was free of ice.
The aircraft was equipped for ice protection with the manufacturer's Known Icing Equipment package, which included pneumatic de-icing boots on the leading edges of the wings and wing struts, horizontal and vertical stabilizers, electrically heated propeller blade anti-ice boots, a detachable electric windshield anti-ice panel, a heated pitot/static system, and a standby electrical system. Engine bleed air supplied heat to the cabin and hot air for the windshield defrost, but the controls were selected to direct hot air to the forward cabin only, and the windshield defrost was not selected. The detachable windshield anti-ice panel was approximately 19 in. high by 9 in. wide.
An area forecast was available to the pilot, and the prognosis for the intended flying area was for cloud to be generally 2500 ft. ASL overcast; visibility 6 SM or greater, with occasional visibility 3 to 6 SM in light snow showers; visibility, at times, ¾ to 3 mi. in light snow showers with stratus/snow ceilings 600 to 1000 ft. ASL; a few stratus cloud ceilings 500 to 1000 ft. ASL; and visibility ½ SM in light freezing drizzle, light drizzle, light freezing fog, light fog in flow off the Great Lakes. Light to moderate rime icing was forecast above the freezing level and moderate mixed icing in light freezing drizzle below 4000 ft. ASL. The freezing level was at or near the surface.
Toronto–Buttonville airport was the closest for which a terminal area forecast (TAF) was available to the pilot. The TAF issued at midnight on March 3 (23:30 EST) called for conditions after 07:00 to be as follows: wind from 040° T at 8 kt., visibility 4 mi. in mist, and cloud 2000 ft. above ground level (AGL) overcast. Conditions were forecast to temporarily fluctuate to visibility 1 mi. in mist with cloud 800 ft. AGL overcast between 07:00 and 12:00.
The final report does not specify whether or not the pilot actually read the area forecast, nor does it specify whether or not he requested updated weather information en route. As far as the investigation could determine, prior to descending on the approach, the pilot did not know freezing drizzle was falling at the airport. Several witnesses reported freezing drizzle at, and in the vicinity of, the Barrie–Orillia airport prior to and at the time the aircraft was on approach.
The VOR/DME final approach radial intersects Runway 10/28 from the southeast at a 29° angle, and requires a circling approach to land in either direction. Runway lighting was available via the aircraft radio control of aerodrome lighting (ARCAL) system, but was not activated by the pilot. The runway was covered with a light dusting of snow and thin film of granular ice at the time the pilot was on approach. No aircraft had landed or departed from the runway on the morning prior to the accident.
The flight was apparently without difficulty until the pilot descended to lower altitudes on approach to the airport, where it is likely that he encountered freezing drizzle below 4000 ft. Flight in freezing drizzle would result in a buildup of clear ice on the unprotected parts of the aircraft and, in particular, on the aircraft windshield. The pilot's forward visibility through the windshield during the later stages of the approach was probably limited to the portion of the windshield protected from ice by the detachable electric windshield anti-ice panel, making any tight circling manoeuvres very risky at best. Ice accumulation on the aircraft airframe would degrade aircraft performance and require that the pilot maintain a higher than normal airspeed on approach.
The grey overcast sky, the reduced flight visibility in freezing drizzle, and the lack of vertical guidance aids on the approach, combined with the light dusting of unbroken snow on the runway, would make it difficult for the pilot to visually judge his height above ground on final approach. After sighting the runway from close to the airport, following an non-precision IFR approach, the pilot elected to manoeuvre the aircraft for an immediate landing on Runway 28. Because of the aircraft's proximity to the runway, the pilot had to carry out a steep, descending left turn to position the aircraft for landing; this is not a recommended manoeuvre during circling approaches. A rapid accumulation of clear ice on the aircraft airframe and the poor visibility may have influenced his decision to attempt an immediate landing instead of carrying out an appropriate circling approach procedure.
Although icing conditions were forecast along the planned route of flight, the report does not discuss the pilot’s pre-flight planning, making it difficult to properly assess his decision to put the aircraft into a forecast icing condition. Nevertheless, it remains the pilot’s responsibility to ascertain whether or not his aircraft was adequately equipped to operate in the forecast conditions. The C208 is certified for flight into known icing conditions according to Chapter 523 of the Airworthiness Manual, which refers to the icing certification criteria contained in the U.S. Federal Aviation Regulations, but those do not cover flight in light freezing drizzle or light freezing fog.
The TSB could not determine why the aircraft struck the ground during the turn to the final approach, but said it was probably because the pilot misjudged his height above ground or because the aircraft stalled since there was ice on the wings. Regardless of the technical and physical reasons for the crash, we cannot help but wonder what other factors led this pilot to operate his aircraft into known icing conditions.
Pressure to complete the flight perhaps? Likely. Why didn’t the pilot use the windshield defrost? Was it because he forgot or because of poor knowledge of his aircraft systems? If he was aware of and understood all of his de-icing equipment, the windshield defrost would definitely have been on. Why didn’t he avail himself of the area forecast? Could it be because he had difficulties interpreting it, like about half the pilots in this country? To think of it, the real causes of this accident have little to do with the final event, and this is why we should all reflect on the buildup to the crash, rather than the outcome.
One last word on area forecasts. How do you feel about them? I would dare to say that most pilots dislike them because it is difficult to interpret or understand them, and mostly, because it is difficult to form a mental picture of the weather situation based on them. Well this is about to change as the current textual format of area forecasts will soon be changed to a graphic description, like a weather observation map, which will make them a lot easier to interpret.
Optical Illusion or Distraction?
On August 10, 1997, a float-equipped Cessna 180, accompanied by an identical Cessna on a fishing trip, crashed on the south slope of the Rivière aux Mélèzes valley in northern Quebec. The pilot and passenger were fatally injured, and the aircraft was destroyed by the post-crash fire. This summary is largely based on Final Report A97Q0168 by the Transportation Safety Board of Canada (TSB).
Both aircraft had taken off around 12:30 p.m. and were flying west over the Rivière aux Mélèzes. The elevation of the valley floor is 300 ft. ASL, and the terrain on both sides of the river rises to at least 1200 ft. ASL. The pilots used a common VHF frequency during the flight. After finding a landing site that appeared suitable, the pilot of the accident aircraft radioed to the other pilot to inspect the site. The latter did a reconnaissance and made a water landing without difficulty. A short time later, the pilot of the accident aircraft initiated a final approach to land at the same spot, but he executed a missed water landing procedure before touching down. He then told the other pilot he was going to examine the landing area more carefully and fly another circuit because he was unsure about the strength of the river current. He climbed above the river to about 450 ft. AGL, then turned 90 degrees left onto the crosswind leg. The aircraft levelled off and proceeded toward the south slope of the valley.
About 30 seconds later, the second pilot saw that the accident aircraft was getting close to the rising terrain and still hadn’t turned parallel to the river and valley wall for the downwind leg. The second pilot suggested he watch out for the mountain. A few seconds later, the aircraft pitched up without changing heading, then made two turns; the first was a right turn at a low bank angle to upwind, and the second was steep and to the left to downwind. The aircraft started to lose altitude and pitched up gradually until it struck some trees, then the ground, in a nose-down attitude. Four or five seconds after the impact, a fire started on the right side of the cabin. Thirty to sixty seconds elapsed between the go-around and the accident.
The accident occurred 100 NM southwest of Kuujjuaq, Quebec, in a partially wooded area approximately one-half mile south of the Rivière aux Mélèzes. The area is somewhat hilly and mainly covered with larch trees of average size. The south side of the valley slopes upward at an angle of about 20 degrees. The aircraft came to rest about 450 ft. above the valley floor. The aircraft cut a swath 50 ft. long through the trees before striking the ground. The impact damage and the nose-down attitude of the wreck are consistent with a loss of control following a stall.
Examination of all recovered components revealed no evidence of pre-impact failure or malfunction, no signs of airframe failure, flight control problems, electrical problems, loss of power, or in-flight fire. No messages were received from the pilot.
According to the TSB report, some situations can severely hinder a pilot's ability to estimate size, distance, speed, or the direction to a slope, or even to identify objects. Pilots can be misled by an optical illusion when approaching rising terrain at right angles. When approaching a ridge, the pilot may tend to maintain a constant angle between the extended cowl and the summit; this causes the pitch attitude of the aircraft to increase while speed decreases. Consequently, aircraft performance decreases and vertical separation with the terrain decreases. The pilot tends to focus on the proximity of the ground, sometimes to the point where flying performance is affected. There is a vivid impression that speed is increasing in relation to the ground, and the pilot may be tempted to reduce speed.
The pilot's decision to fly a left-hand circuit was sound, since he was in the left seat and visibility was better on that side. As the purpose of the reconnaissance was to examine the surface of the water, the pilot had to fly at low level and low speed.
With the aircraft in approximately level flight, it must have closed rapidly with the rising terrain. The pilot did not fly close to the north side of the valley before turning onto the crosswind leg, and as a result, he did not take advantage of all the available airspace in case he needed it. Consequently, not all the space available for the circuit was used to minimize roll attitude in the turns and maximize aircraft performance. The type of circuit selected indicated the pilot intended to do a landing area reconnaissance at low altitude.
Flying in mountainous terrain demands heightened vigilance. Pilots must constantly confirm their impressions with instrument readings. The TSB was unable to determine why the pilot continued flying towards the slope at right angles instead of trying to avoid the ridge until the second pilot warned him. Two hypotheses might explain the pilot's delay in turning onto the downwind leg: he may have been distracted, and/or he may have been misled by optical illusions.
One hypothesis is that the pilot’s attention may have been focussed on planning the water landing or on an untimely event in the cabin. It is possible that, after the go-around, most of his attention was focussed on a continuous examination of the landing area to his left and slightly behind him, and not on flying the circuit. Also, a distraction caused by the passenger feeling the effects of motion sickness or being otherwise indisposed could have produced the same result.
The other hypothesis is that, while flying towards the rising slope, the pilot may have been tricked by an optical illusion, which can be treacherous at low altitude and at near-stall speeds.
After the second pilot called to tell him to watch out for the mountain, the accident aircraft pilot seemed to react, but he did not have much time and his room to manoeuvre may have been reduced to the point where turning around would cause a stall in the turn. The pilot may have assessed the situation and decided to terminate the flight immediately with a forced landing in the best available conditions on the slope of the valley.
The pilot apparently did not have time to cut electrical power and fuel and prepare the cabin for rapid evacuation. Based on the evidence and witness statements, the cause of the accident could not be determined.
Damage to the right wing caused a fuel leak, and, on contact with an ignition source, the fuel ignited and sustained the fire. The witness statements and fire damage suggested that the fire started on the right side of the cabin and the most likely ignition source was electrical; however, the investigation could not identify the source of ignition with certainty.
As a result, the TSB determined that an unknown distraction and/or an optical illusion may have contributed to diverting the pilot's attention from flying the circuit. Although the cause of this accident was not determined, the conditions were conducive to optical illusions associated with flying over rising terrain at low altitude.
Good Judgement Overruled
There are times when you just don't take off. There is no question about it, no thought needed, when, for example, the weather is totally outrageous, the airplane is not really airworthy or some other problem exists that makes [the] proposed flight just downright dangerous. Every pilot is confronted with such circumstances every so often. There is little doubt about what could happen if the airplane leaves the ground that day.
Brian Jacobson corporate pilot and Contributing Editor to Aviation Safety magazine
One pilot's reason for departing VFR into instrument meteorological conditions was that he needed to get his Piper Archer from airport A to airport B 14 mi. away to have it repaired so that he could leave for Florida the next morning.
He had had a total electrical failure the previous day while practising instrument approaches with a friend. He was recharging the battery but needed to get his alternator repaired. The problem was that the weather was solid IFR.
When he called the FSS that morning for a weather briefing, he explained to the specialist that, while he held an IFR rating (having 600 hrs' total time, of which 60 hrs were instrument time and 370 hrs were on type), he could not file an instrument flight plan because of his electrical problem. If he were flying VFR, he could use battery power for his radio and transponder to enter the Class C airspace at airport B.
The weather at B was 300 ft. overcast, with visibility 0.75 mi. in light rain, and forecast to stay that way until evening. The briefer told the pilot that VFR was not recommended.
The pilot explained that he needed to get to B for repairs since he was leaving early the next morning for Florida. "Well, the thing is, if I could fly there IFR... but it's just not legal for me to do that, you see, with only the battery working."
"The alternator is completely out, and I don't know how long the battery is going to last, much less if I'll get the airplane started."
"I guess I'll check with you again, maybe around noon. When will this be updated?"
The pilot's urgency was evident in the conversation. When he called back, he repeated his story about the alternator failure and the need to fly VFR to B for repairs. The updated forecast for B called for 500 ft. overcast and visibility 2 mi. for the rest of the day and evening. He told the briefer that he would be in touch with the tower at B in case the weather improved enough for him to get there.
When he called the briefer back a third time just before 5 p.m., he told much the same story, but this time, instead of saying that he needed VFR, he said, "I have to get special VFR." He had decided to go regardless of the weather.
The briefer advised him to wait until morning, when the weather would improve. The actual weather at B was 300 ft. overcast and visibility 2 mi., with the forecast not much better for the rest of the night. The pilot thanked the briefer, hung up and called the tower at B. He advised the controller of his need to get special VFR into the control zone. After confirming that he had a radio, the tower controller advised him to contact the terminal controller after takeoff to make his request.
The pilot did that just about an hour later. He was given a transponder code, identified on radar and advised that there would be a 5-min. delay because instrument approaches were in progress at B. When the clearance was given, the pilot asked for a heading to the airport. He was assigned a vector.
A Cessna 421 pilot flying the ILS approach at B overheard the conversation. When he checked in on the tower frequency, he advised that conditions on final were not conducive to special VFR. That information was passed on to the arrival controller handling the Archer.
When told that the ceiling on final at B was 300 ft., the Archer pilot replied, "Well, I guess it's too late for me to go back. So, I'll fly the approach, okay?" Since only 14 mi. separated the two airports, it is likely that the weather was just as bad at his uncontrolled departure airport, and there was no instrument approach.
He was given a vector for the ILS localizer. He flew through the localizer and, when queried by the controller, acknowledged that he was turning to intercept. The controller noted that he was intercepting the on-course and the pilot agreed. Less than a minute later, the pilot advised that he was having a gyro problem. "It's all mixed up," he said.
The controller immediately responded by telling the pilot to climb to 3000 ft. The pilot acknowledged, but added, "I'm going to lose communication pretty soon. My battery is pretty bad." The controller intended to provide a surveillance no-gyro approach and he began giving directions to turn, stating when to start the turn and when to stop. The static-filled transmission "DG not working" was the last from the aircraft. It crashed in a residential area, killing the pilot. No one on the ground was hurt.
Including the time required for engine start-up, the aircraft had been operating at power for about 30 min. when it crashed.
Investigators found no indication that the gyro was not operating normally at impact. Even without communication or navigation capability, the pilot should have been able to fly the aircraft. However, it is possible that, in the high-stress situation, he started to overcontrol the aircraft to the point where he thought that the instruments were malfunctioning. When he stopped believing and scanning his instruments, he apparently became disoriented and lost control.
A 14-mi. trip in good VFR conditions would not likely have caused any difficulties, even on questionable battery power; however, the weather for the attempted flight was not "good VFR." It had been reported at 300 ft. overcast with visibility 2 mi. most of the day. Waiting until the following morning to ferry the aircraft to airport B to get the alternator replaced would have cost the pilot a couple of hours' delay in the start of his Florida trip.
When forced by the weather to fly a full instrument approach on a fading battery, the pilot knew that he had a serious emergency, and he should have declared it. The controller knew about the aircraft's mechanical conditions, but reasonably expected the pilot to have enough battery power available to do what was expected during the flight. Since the pilot did not declare the emergency, the flight was treated in a routine manner. Had the controller known that an emergency existed, he could have assisted by turning him in early for the ILS approach or perhaps immediately giving vectors for the surveillance approach.
The accident should not have happened. It happened because the pilot convinced himself that it was acceptable to take a questionable aircraft through poor weather to save a couple of hours. His good judgement was overruled by the self-imposed pressure to get an early start the next day.
Human factors experts would call it an example of a mental "trap" known as a "framing bias."
One of the things that contributed to the poor judgement illustrated in this accident is the way that a problem is framed. In risky decision making, there is a tendency to frame the problem as a choice between gains and losses.
With respect to lossed, people are biased to chance the risky loss, which they see as less probable, although more disastrous, than the certain loss.
Think about which way your bias is!
Originally Published: ASL 4/1997
Original Article: Good Judgement Overruled













Pilot Resources
Ask ATS
Weather
TSB
Interactive Materials
NOTAMs
Air Safety Institute
ELTs
Aviation Safety Letter
SmartPilot proudly works with.


We would like to acknowledge the financial support of the Government of Canada for this initiative through the Search and Rescue New Initiative Fund (SAR NIF).